
Tube Surgery
Tube Surgery also known as ‘Glaucoma drainage device’ surgery, is used in the treatment of glaucoma by surgically lowering the internal eye pressure. Generally speaking, it is usually reserved for patients that have previously failed treatment with other types of glaucoma surgery such as trabeculectomy or for glaucoma caused by other eye diseases (e.g. uveitis, neovascular, trauma, previous retinal or corneal surgery).
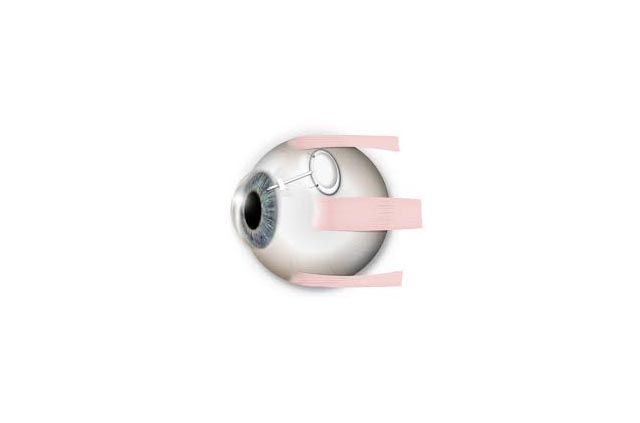
The picture to the right demonstrates location of the tube within the ‘anterior chamber’ of the eye.
How is the surgery performed?
Tube surgery is usually performed under general anaesthesia (i.e. put to sleep). The device consists of a very small and delicate silicone tube that is inserted into the front chamber of the eye. The fluid within the eye is drained via the tube to the ‘plate’ portion of the silicone device which is implanted outside the eye, thus lowering the internal eye pressure (figure 2a & 2b, below). The device itself is then covered by conjunctiva (the mucous membrane that normally wraps around the white of the eye). In addition, most surgeons will also use extra material (such as donor sclera) to cover the tube implant in order to reduce the risk of future erosion exposure.
What to expect after the procedure?
Depending on the type of tube device used, post-operative progress during the initial few weeks may differ slightly. Devices that have built-in ‘valve’ mechanisms (such as the Ahmed valve) allows lower pressure immediately. Other ‘non-valved’ designs offer better long-term pressure control, but the tube is deliberately tied shut and only partially effective during the first 6 weeks; after which the self-dissolvable tie loosens and the tube fully opens. Success rate is around 80%. Further procedures may be required for those with insufficient pressure lowering from the surgery. Your intraocular pressures will be regularly monitored during this post-operative period.
Figure 2a

Figure 2b
What are the risks of Tube Surgery?
All surgeries carry some risks, and any operation is not done unless the chance of benefit outweighs the risk. Common expected side effects such as redness, grittiness and mild to moderate blurring are usually transient. The risk of severe complications causing irreversible loss of vision is very low (1 in 1000). These include infection and expulsive haemorrhage. Other less serious complications include: transient hypotony where the internal eye pressure becomes too low from over-drainage, decompensation of the cornea, persistent double vision, formation of cataract and drooping of the eye lids.
If you would like to discuss about tube surgery further, please do not hesitate to consult with one of our doctors at Applecross Eye Clinic.